

Child Death Review
Overview
This section sets out the work of the Office in relation to its child death review function. Information on this work has been set out as follows:
- Background;
- The role of the Ombudsman in relation to child death reviews;
- The child death review process;
- Analysis of child death reviews;
- Patterns, trends and case studies relating to child death reviews;
- Issues identified in child death reviews;
- Recommendations;
- Major own motion investigations arising from child death reviews;
- Other mechanisms to prevent or reduce child deaths; and
- Stakeholder liaison.
Background
In November 2001, prompted by the coronial inquest into the death of a 15 year old Aboriginal girl at the Swan Valley Nyoongar Community in 1999, the (then) State Government announced a special inquiryinto the response by government agencies to complaints of family violence and child abuse in Aboriginal communities.
The resultant 2002 report, Putting the Picture Together: Inquiry into Response by Government Agencies to Complaints of Family Violence and Child Abuse in Aboriginal Communities, recommended that a Child Death Review Team be formed to review the deaths of children in Western Australia (Recommendation 146). Responding to the report the (then) Government established the Child Death Review Committee (CDRC), with its first meeting held in January 2003. The function of the CDRC was to review the operation of relevant policies, procedures and organisational systems of the (then) Department for Community Development in circumstances where a child had contact with the Department.
In August 2006, the (then) Government announced a functional review of the (then) Department for Community Development. Ms Prudence Ford was appointed the independent reviewer and presented the report, Review of the Department for Community Development: Review Report (the Ford Report) to the (then) Premier in January 2007. In considering the need for an independent, inter-agency child death review model, the Ford Report recommended that:
- The CDRC together with its current resources be relocated to the Ombudsman (Recommendation 31); and
- A small, specialist investigative unit be established in the Office to facilitate the independent investigation of complaints and enable the further examination, at the discretion of the Ombudsman, of child death review cases where the child was known to a number of agencies (Recommendation 32).
Subsequently, the Parliamentary Commissioner Act 1971 was amended to enable the Ombudsman to undertake child death reviews, and on 30 June 2009, the child death review function in the Office commenced operation.
The Role of the Ombudsman in relation to Child Death Review
The child death review function enables the Ombudsman to review investigable deaths. Investigable deaths are defined in the Ombudsman’s legislation, the Parliamentary Commissioner Act 1971 (see Section 19A(3)),and occur when a child dies in any of the following circumstances:
- In the two years before the date of the child’s death:
- The Chief Executive Officer (CEO) of the Department of Communities (Communities) had received information that raised concerns about the wellbeing of the child or a child relative of the child;
- Under section 32(1) of the Children and Community Services Act 2004, the CEO had determined that action should be taken to safeguard or promote the wellbeing of the child or a child relative of the child; and
- Any of the actions listed in section 32(1) of the Children and Community Services Act 2004 was done in respect of the child or a child relative of the child.
- The child or a child relative of the child is in the CEO’s care or protection proceedings are pending in respect of the child or a child relative of the child.
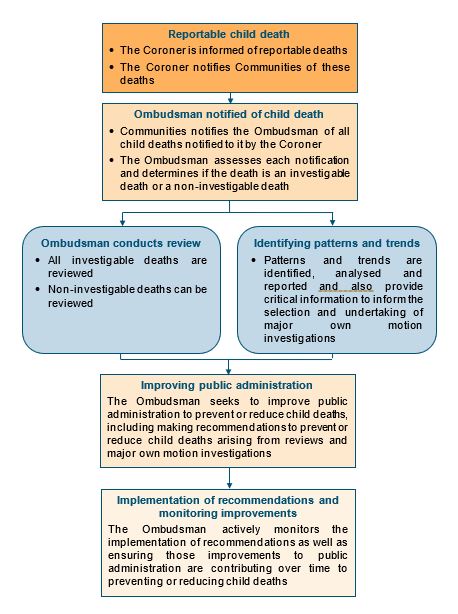
In particular, the Ombudsman reviews the circumstances in which and why child deaths occur, identifies patterns and trends arising from child deaths and seeks to improve public administration to prevent or reduce child deaths.
In addition to reviewing investigable deaths, the Ombudsman can review other notified deaths. The Ombudsman also undertakes major own motion investigations arising from child death reviews.
In reviewing child deaths the Ombudsman has wide powers of investigation, including powers to obtain information relevant to the death of a child and powers to recommend improvements to public administration about ways to prevent or reduce child deaths across all agencies within the Ombudsman’s jurisdiction. The Ombudsman also has powers to monitor the steps that have been taken, are proposed to be taken or have not been taken to give effect to the recommendations.
The Child Death Review Process
Analysis of Child Death Reviews
By reviewing child deaths, the Ombudsman is able to identify, record and report on a range of information and analysis, including:
- The number of child death notifications and reviews;
- The comparison of investigable deaths over time;
- Demographic information identified from child death reviews;
- Circumstances in which child deaths have occurred;
- Social and environmental factors associated with investigable child deaths;
- Analysis of children in particular age groups; and
- Patterns, trends and case studies relating to child death reviews.
Notifications and Reviews
Communities receives information from the Coroner on reportable deaths of children and notifies the Ombudsman of these deaths. The notification provides the Ombudsman with a copy of the information provided to Communities by the Coroner about the circumstances of the child’s death together with a summary outlining the past involvement of Communities with the child and the child’s family.
The Ombudsman assesses all child death notifications received to determine if the death is, or is not, an investigable death. If the death is an investigable death, it must be reviewed. If the death is a non-investigable death, it can be reviewed. The extent of a review depends on a number of factors, including the circumstances surrounding the child’s death and the level of involvement of Communities or other public authorities in the child’s life. Confidentiality of the child, family members and other persons involved with the case is strictly observed.
The child death review process is intended to identify key learnings that will positively contribute to ways to prevent or reduce child deaths. The review does not set out to establish the cause of the child’s death; this is properly the role of the Coroner.
Child death review cases prior to 30 June 2009
At the commencement of the child death review jurisdiction on 30 June 2009, 73 cases were transferred to the Ombudsman from the CDRC. These cases related to child deaths prior to 30 June 2009 that were reviewable by the CDRC and covered a range of years from 2005 to 2009. Almost all (67 or 92%) of the transferred cases were finalised in 2009-10 and six cases were carried over. Three of these transferred cases were finalised during 2010-11 and the remaining three were finalised in 2011-12.
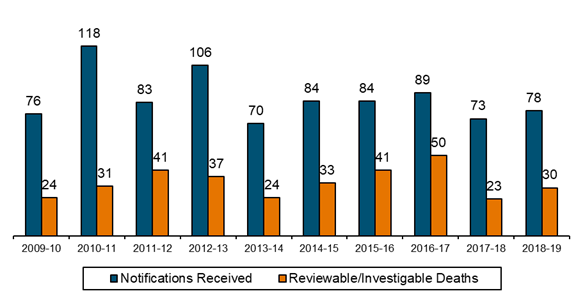
Number of child death notifications and reviews
During 2018-19, there were 30 child deaths that were investigable and subject to review from a total of 78 child death notifications received.
Total Number of Notifications Received 2009-10 to 2018-19 |
|
Comparison of investigable deaths over time
The Ombudsman commenced the child death review function on 30 June 2009. Prior to that, child death reviews were undertaken by the CDRC with the first full year of operation of the CDRC in 2003-04.
The following table provides the number of deaths that were determined to be investigable by the Ombudsman or reviewable by the CDRC compared to all child deaths in Western Australia for the 16 years from 2003-04 to 2018-19. It is important to note that an investigable death is one which meets the legislative criteria and does not necessarily mean that the death was preventable, or that there has been any failure of the responsibilities of Communities.
Comparisons are also provided with the number of child deaths reported to the Coroner and deaths where the child or a relative of the child was known to Communities. It should be noted that children or their relatives may be known to Communities for a range of reasons.
Year |
A |
B |
C |
D |
Total WA child deaths |
Child deaths reported |
Child deaths where the child or a relative of the child was known to Communities |
Reviewable/ investigable child deaths |
|
2003-04 |
177 |
92 |
42 |
19 |
2004-05 |
212 |
105 |
52 |
19 |
2005-06 |
210 |
96 |
55 |
14 |
2006-07 |
165 |
84 |
37 |
17 |
2007-08 |
187 |
102 |
58 |
30 |
2008-09 |
167 |
84 |
48 |
25 |
2009-10 |
201 |
93 |
52 |
24 |
2010-11 |
203 |
118 |
60 |
31 |
2011-12 |
150 |
76 |
49 |
41 |
2012-13 |
193 |
121 |
62 |
37 |
2013-14 |
156 |
75 |
40 |
24 |
2014-15 |
170 |
93 |
48 |
33 |
2015-16 |
178 |
92 |
61 |
41 |
2016-17 |
181 |
91 |
60 |
50 |
2017-18 |
138 |
81 |
37 |
23 |
2018-19 |
165 |
81 |
37 |
30 |
Notes
- The data in Column A has been provided by the Registry of Births, Deaths and Marriages. Child deaths within each year are based on the date of death rather than the date of registration of the death. The CDRC included numbers based on dates of registration of child deaths in their Annual Reports in the years 2005-06 through to 2007-08 and accordingly the figures in Column A will differ from the figures included in the CDRC Annual Reports for these years because of the difference between dates of child deaths and dates of registration of child deaths. The data in Column A is subject to updating and may vary from data published in previous Annual Reports.
- The data in Column B has been provided by the Office of the State Coroner. Reportable child deaths received by the Coroner are deaths reported to the Coroner of children under the age of 18 years pursuant to the provisions of the Coroners Act 1996. The data in this section is based on the number of deaths of children that were reported to the Coroner during the year.
- ‘Communities’ refers to the Department of Communities from 2017-18, Department for Child Protection and Family Support for the year 2012-13 to 2016-17, Department for Child Protection for the years 2006-07 to 2011-12 and Department for Community Development (DCD) prior to 2006-07. The data in Column C has been provided by Communities and is based on the date the notification was received by Communities. For 2003-04 to 2007-08 this information is the same as that included in the CDRC Annual Reports for the relevant year. In the 2005-06 to 2007-08 Annual Reports, the CDRC counted ‘Child death notifications where any form of contact had previously occurred with Communities: recent, historical, significant or otherwise’. In the 2003-04 and 2004-05 Annual Reports, the CDRC counted ‘Coroner notifications where the families had some form of contact with DCD’.
- The data in Column D relates to child deaths considered reviewable by the CDRC up to
30 June 2009 or child deaths determined to be investigable by the Ombudsman from 30 June 2009. It is important to note that reviewable deaths and investigable deaths are not the same, however, they are similar in effect. The definition of reviewable death is contained in the Annual Reports of the CDRC. The term investigable death has the meaning given to it under section 19A(3) of the Parliamentary Commissioner Act 1971. - The number of investigable child deaths shown in a year may vary, by a small amount, from the number shown in previous annual reports for that year. This occurs because, after the end of the reporting period, further information may become available that requires a reassessment of whether or not the death is an investigable death. Since the commencement of the child death review function this has occurred on one occasion resulting in the 2009-10 number of investigable deaths being revised from 23 to 24.
Demographic information identified from child death reviews
Information is obtained on a range of characteristics of the children who have died including gender, Aboriginal status, age groups and residence in the metropolitan or regional areas. A comparison between investigable and non-investigable deaths can give insight into factors that may be able to be affected by Communities in order to prevent or reduce deaths.
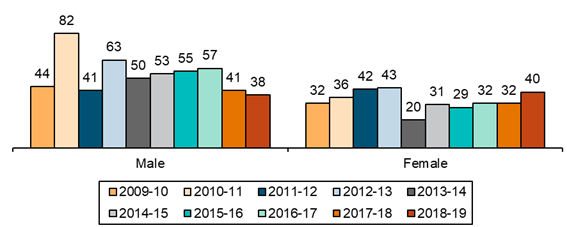
The following charts show:
- The number of children in each group for each year from 2009-10 to 2018-19; and
- For the period from 30 June 2009 to 30 June 2019, the percentage of children in each group for both investigable deaths and non-investigable deaths, compared to the child population in Western Australia.
Males and females
As shown in the following charts, considering all 10 years, male children are over‑represented compared to the population for both investigable and non‑investigable deaths.
Number of Notifications by Gender |
| Title Text (Note - you have to use hard returns at the end of each paragraph otherwise it turns the text to paragraph font which you do not want). |
Go to next section of the Annual Report 2018-19 >>
Go to previous section of the Annual Report 2018-19>>
Go back to Annual Reports page >>
To read a pdf, you will need Adobe Acrobat Reader, which can be downloaded
for free from Adobe at http://www.adobe.com/products/
acrobat/readstep2.html.