

Child Death Review
This section sets out the work of the Office in relation to its child death review function. Information on this work has been divided as follows:
- Background;
- The role of the Office in child death reviews;
- The child death review process;
- Notifications and reviews;
- Patterns and trends identified from child death reviews;
- Improvements to public administration to prevent or reduce child deaths; and
- Stakeholder liaison.
Background
In November 2001, prompted by the coronial inquest into the death of a 15 year old Aboriginal girl at the Swan Valley Nyoongar Community in 1999, the (then) Government announced a special inquiryinto the response by Government agencies to complaints of family violence and child abuse in Aboriginal communities.
The resultant 2002 report, Putting the Picture Together: Inquiry into Response by Government Agencies to Complaints of Family Violence and Child Abuse in Aboriginal Communities, recommended that a Child Death Review Team be formed to review the deaths of children in Western Australia (Recommendation 146). Responding to the report the (then) Government established the Child Death Review Committee (CDRC), with its first meeting held in January 2003. The function of the CDRC was to review the operation of relevant policies, procedures and organisational systems of the (then) Department for Community Development in circumstances where a child had contact with the Department.
In August 2006, the (then) Government announced a functional review of the (then) Department for Community Development. Ms Prudence Ford was appointed the independent reviewer and presented the report, Review of the Department for Community Development: Review Report (the Ford Report) to the (then) Premier in January 2007. In considering the need for an independent, inter-agency child death review model, the Ford Report recommended that:
- The CDRC together with its current resources be relocated to the Ombudsman (Recommendation 31); and
- A small, specialist investigative unit be established in the Office to facilitate the independent investigation of complaints and enable the further examination, at the discretion of the Ombudsman, of child death review cases where the child was known to a number of agencies (Recommendation 32).
Subsequently, the Parliamentary Commissioner Act 1971 was amended to enable the Ombudsman to undertake child death reviews, and on 30 June 2009, the child death review function in the Office commenced operation.
The Role of the Office in Child Death Reviews
The child death review function enables the Ombudsman to review investigable deaths. Investigable deaths are defined in the Ombudsman’s legislation, the Parliamentary Commissioner Act 1971 (see Section 19A(3)),and occur when a child dies in any of the following circumstances:
- In the two years before the date of the child’s death:
- The Chief Executive Officer (CEO) of the Department for Child Protection and Family Support (DCPFS) had received information that raised concerns about the wellbeing of the child or a child relative of the child;
- Under section 32(1) of the Children and Community Services Act 2004, the CEO had determined that action should be taken to safeguard or promote the wellbeing of the child or a child relative of the child; and
- Any of the actions listed in section 32(1) of the Children and Community Services Act 2004 was done in respect of the child or a child relative of the child.
- The child or a child relative of the child is in the CEO’s care or protection proceedings are pending in respect of the child or a child relative of the child.
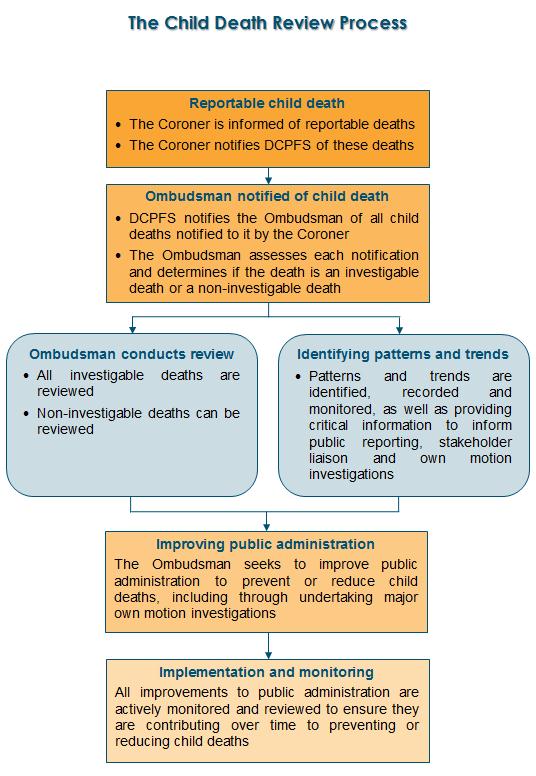
In particular, the Ombudsman reviews the circumstances in which and why child deaths occur, identifies patterns and trends arising from child deaths and seeks to improve public administration to prevent or reduce child deaths.
In addition to reviewing investigable deaths, the Ombudsman can review other notified deaths. The Ombudsman also undertakes major own motion investigations arising from child death reviews.
In reviewing child deaths the Ombudsman has wide powers of investigation, including powers to obtain information relevant to the death of a child and powers to recommend improvements to public administration about ways to prevent or reduce child deaths across all agencies within the Ombudsman’s jurisdiction.
| The Ombudsman reviews certain child deaths, identifies patterns and trends arising from these deaths and seeks to improve public administration to prevent or reduce child deaths, including through the undertaking of major own motion investigations. |
Notifications and Reviews
DCPFS receives information from the Coroner on reportable deaths of children and notifies the Ombudsman of these deaths. The notification provides the Ombudsman with a copy of the information provided to DCPFS by the Coroner about the circumstances of the child’s death together with a summary outlining the past involvement of DCPFS with the child.
The Ombudsman assesses all child death notifications received to determine if the death is, or is not, an investigable death. If the death is an investigable death, it must be reviewed. If the death is a non-investigable death, it can be reviewed. The extent of a review depends on a number of factors, including the circumstances surrounding the child’s death and the level of involvement of DCPFS or other public authorities in the child’s life. Confidentiality of the child, family members and other persons involved with the case is strictly observed.
The child death review process is intended to identify key learnings that will positively contribute to ways to prevent or reduce child deaths. The review does not set out to establish the cause of the child’s death; this is properly the role of the Coroner.
Child death review cases prior to 30 June 2009
At the commencement of the child death review jurisdiction on 30 June 2009, 73 cases were transferred to the Ombudsman from the CDRC. These cases related to child deaths prior to 30 June 2009 that were reviewable by the CDRC and covered a range of years from 2005 to 2009. Almost all (67 or 92%) of the transferred cases were finalised in 2009-10 and six cases were carried over. Three of these transferred cases were finalised during 2010-11 and the remaining three were finalised in 2011‑12.
Number of child death notifications and reviews
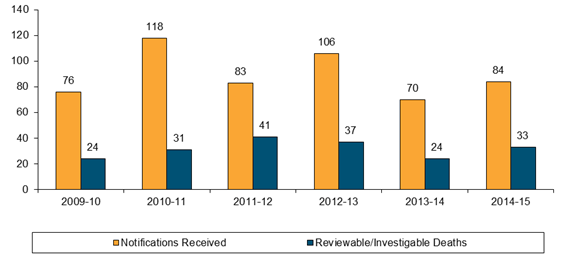
During 2014-15, there were 33 child deaths that were investigable and subject to review from a total of 84 child death notifications received.
| Total Number of Notifications Received 2009-10 to 2014-15 |
|
Comparison of investigable deaths over time
The Ombudsman commenced the child death review function on 30 June 2009. Prior to that, child death reviews were undertaken by the CDRC with the first full year of operation of the CDRC in 2003-04.
The following table provides the number of deaths that were determined to be investigable by the Ombudsman or reviewable by the CDRC compared to all child deaths in Western Australia for the 12 years from 2003-04 to 2014-15. It is important to note that an investigable death is one which meets the legislative criteria and does not necessarily mean that the death was preventable, or that there has been any failure of the responsibilities of DCPFS.
Comparisons are also provided with the number of child deaths reported to the Coroner and deaths where the child or a relative of the child was known to DCPFS. It should be noted that children or their relatives may be known to DCPFS for a range of reasons.
Year |
A |
B |
C |
D |
Total WA child deaths (See Note 1) |
Child deaths reported (See Note 2) |
Child deaths where the child or a relative of the child was known to DCPFS (See Note 3) |
Reviewable/ investigable child deaths (See Note 4 and Note 5) |
|
2003-04 |
177 |
92 |
42 |
19 |
2004-05 |
212 |
105 |
52 |
19 |
2005-06 |
210 |
96 |
55 |
14 |
2006-07 |
165 |
84 |
37 |
17 |
2007-08 |
187 |
102 |
58 |
30 |
2008-09 |
167 |
84 |
48 |
25 |
2009-10 |
201 |
93 |
52 |
24 |
2010-11 |
199 |
118 |
60 |
31 |
2011-12 |
144 |
76 |
49 |
41 |
2012-13 |
189 |
121 |
62 |
37 |
2013-14 |
151 |
75 |
40 |
24 |
2014-15 |
157 |
93 |
48 |
33 |
Abbreviations
DCPFS: Department for Child Protection and Family Support from 2012-13, Department for Child Protection for the years 2006-07 to 2011-12 and Department for Community Development (DCD) prior to 2006-07.
Notes
- The data in Column A has been provided by the Registry of Births, Deaths and Marriages. Child deaths within each year are based on the date of death rather than the date of registration of the death. The CDRC included numbers based on dates of registration of child deaths in their Annual Reports in the years 2005-06 through to 2007-08 and accordingly the figures in Column A will differ from the figures included in the CDRC Annual Reports for these years because of the difference between dates of child deaths and dates of registration of child deaths.
- The data in Column B has been provided by the Office of the State Coroner. Reportable child deaths received by the Coroner are deaths reported to the Coroner of children under the age of 18 years pursuant to the provisions of the Coroners Act 1996. The data in this section is based on the number of deaths of children that were reported to the Coroner during the year.
- The data in Column C has been provided by DCPFS and is based on the date the notification was received by DCPFS. For 2003-04 to 2007-08 this information is the same as that included in the CDRC Annual Reports for the relevant year. In the 2005-06 to 2007-08 Annual Reports, the CDRC counted ‘Child death notifications where any form of contact had previously occurred with DCPFS: recent, historical, significant or otherwise’. In the 2003-04 and 2004-05 Annual Reports, the CDRC counted ‘Coroner notifications where the families had some form of contact with DCD’.
- The data in Column D relates to child deaths considered reviewable by the CDRC up to
30 June 2009 or child deaths determined to be investigable by the Ombudsman from
30 June 2009. It is important to note that reviewable deaths and investigable deaths are not the same, however, they are similar in effect. The definition of reviewable death is contained in the Annual Reports of the CDRC. The term investigable death has the meaning given to it under section 19A(3) of the Parliamentary Commissioner Act 1971. - The number of investigable child deaths shown in a year may vary, by a small amount, from the number shown in previous annual reports for that year. This occurs because, after the end of the reporting period, further information may become available that requires a reassessment of whether or not the death is an investigable death. Since the commencement of the child death review function this has occurred on one occasion resulting in the 2009-10 number of investigable deaths being revised from 23 to 24.
Timely handling of notifications and reviews
The Office places a strong emphasis on the timely review of child deaths. This ensures reviews contribute, in the most timely way possible, to the prevention or reduction of future deaths. In 2014-15, timely review processes have resulted in nearly 90% of all reviews being completed within six months.
Patterns and Trends Identified from Child Death Reviews
By examining all child death notifications, the Ombudsman is able to capture data relating to demographics, risk factors and social and environmental characteristics and identify patterns and trends in relation to child deaths. When child death notifications are finalised, all relevant issues are identified and recorded and, over time, indicate relevant patterns and trends in relation to the issues associated with child deaths. These patterns and trends are identified, recorded, monitored, reported and analysed. They also provide critical information for own motion investigations, including Planning for children in care: An Ombudsman’s own motion investigation into the administration of the care planning provisions of the Children and Community Services Act 2004, which was tabled in Parliament in November 2011; Investigation into ways that State Government departments can prevent or reduce sleep-related infant deaths, which was tabled in Parliament in November 2012; and the Investigation into ways that State Government departments and authorities can prevent or reduce suicide by young people, which was tabled in Parliament in April 2014. In 2014-15, the Office commenced a major own motion investigation into ways to prevent or reduce child deaths by drowning.
Characteristics of children who have died
Information is obtained on a range of characteristics of the children who have died including gender, Aboriginal status, age groups and residence in the metropolitan or regional areas. A comparison between investigable and non-investigable deaths can give insight into factors that may be able to be affected by DCPFS in order to prevent or reduce deaths.
The following charts show:
- The number of children in each group for each year from 2009-10 to 2014-15; and
- For the period from 30 June 2009 to 30 June 2015, the percentage of children in each group for both investigable deaths and non-investigable deaths, compared to the child population in Western Australia.
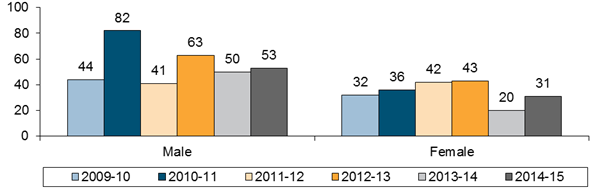
Males and females
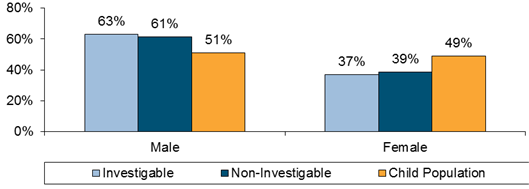
As shown in the following charts, considering all six years, male children are over‑represented compared to the population for both investigable and non‑investigable deaths.
| Number of Notifications by Gender
|
| % of Notifications from 30.6.09 to 30.6.15 Compared to Child Population |
|
Further analysis of the data shows that, considering all six years, male children are over-represented for all age groups, but particularly for children under the age of one and children aged between six and 12 years.
Aboriginal status
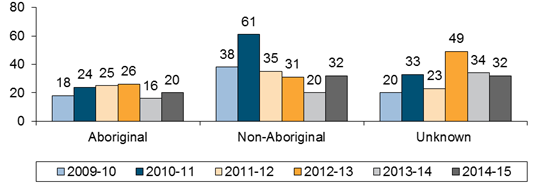
As shown in the following charts, Aboriginal children are over-represented compared to the population in all deaths and more so for investigable deaths.
Number of Notifications by Aboriginal Status |
|
| % of Notifications from 30.6.09 to 30.6.15 Compared to Child Population |
|
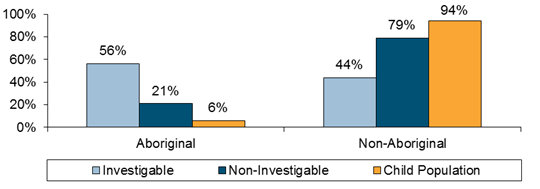
Note: Percentages for each group are based on the percentage of children whose Aboriginal status is known. Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available on the Aboriginal status of the child.
Further analysis of the data shows that Aboriginal children are more likely than non-Aboriginal children to be under the age of one and living in regional and remote locations.
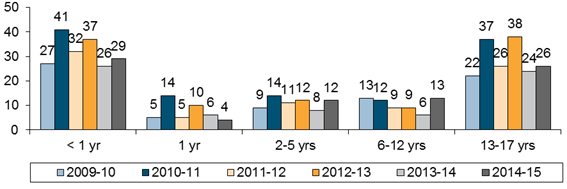
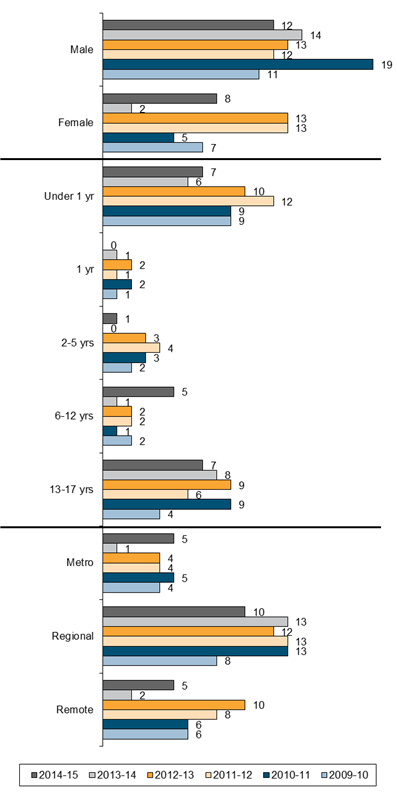
Age groups
As shown in the following charts, children under one year and children aged between 13 and 17 are over-represented compared to the child population as a whole for both investigable and non-investigable deaths.
Number of Notifications by Age of Child |
|
% of Notifications from 30.6.09 to 30.6.15 Compared to Child Population |
|
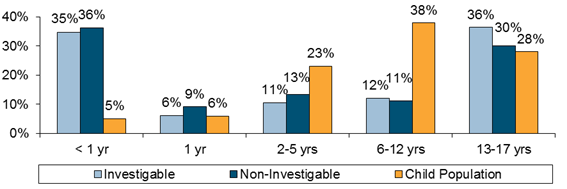
Further analysis of the data shows that Aboriginal children are more likely to be under the age of one than non-Aboriginal children. A more detailed analysis by age group is provided later in this section.
Location of residence
As shown in the following charts, children in regional locations are over-represented compared to the child population as a whole, and more so for investigable deaths.
Number of Notifications by Location of Child |
|
Note: Outside WA includes children whose residence is not in Western Australia, but the child died in Western Australia. Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available on the place of residence of the child.
% of Notifications from 30.6.09 to 30.6.15 Compared to Child Population |
|
Further analysis of the data shows that 82% of Aboriginal children who died were living in regional or remote locations when they died. Most non-Aboriginal children who died lived in the metropolitan area but the proportion of non-Aboriginal children who died in regional areas is higher than would be expected based on the child population.
Circumstances of child deaths
The child death notification received by the Ombudsman includes general information on the circumstances of death. This is an initial indication of how the child may have died but is not the cause of death, which can only be determined by the Coroner. The Ombudsman’s review of the child death will normally be finalised prior to the Coroner’s determination of cause of death.
The circumstances of death are categorised by the Ombudsman as:
- Sudden unexpected death of an infant – that is, infant deaths in which the likely cause of death cannot be explained immediately;
- Motor vehicle accident – the child may be a pedestrian, driver or passenger;
- Illness or medical condition;
- Suicide;
- Drowning;
- Accident other than motor vehicle – this includes accidents such as house fires, electrocution and falls;
- Alleged homicide; and
- Other.
The following chart shows the circumstances of notified child deaths over the last six years.
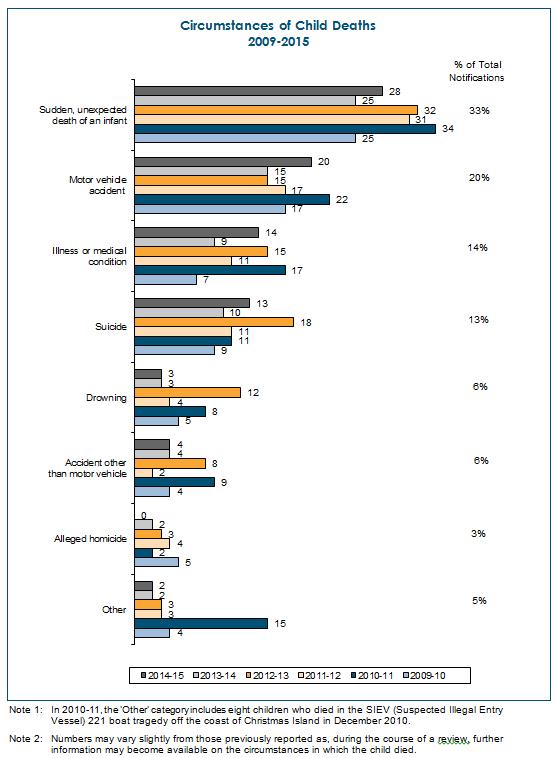
The two main circumstances of death for the 537 child death notifications received in the six years from 30 June 2009 to 30 June 2015 are:
- Sudden, unexpected deaths of infants, representing 33% of the total child death notifications from 30 June 2009 to 30 June 2015 (33% of the child death notifications received in 2009-10, 29% in 2010-11, 37% in 2011-12, 30% in
2012-13, 36% in 2013-14, and 33% in 2014-15); and - Motor vehicle accidents, representing 20% of the total child death notifications from 30 June 2009 to 30 June 2015 (22% of the child death notifications received in 2009-10, 19% in 2010-11, 20% in 2011-12, 14% in 2012-13, 21% in 2013-14, and 24% in 2014-15).
The following chart provides a breakdown of the circumstances of death for child death notifications for investigable and non-investigable deaths.
Circumstances of Child Deaths % of Total Child Death Notifications from 30.6.09 to 30.6.15 |
|
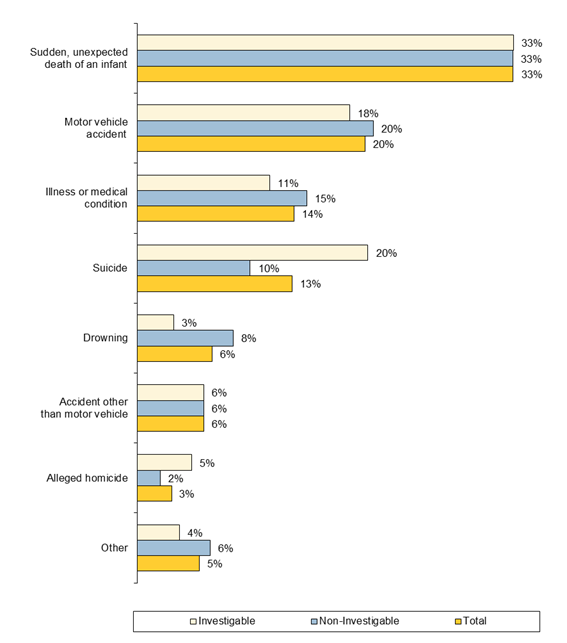
There are two areas where the circumstance of death shows a higher proportion for investigable deaths than for deaths that are not investigable. These are:
- Suicide; and
- Alleged homicide.
Longer term trends in the circumstances of death
The CDRC also collated information on child deaths, using similar definitions, for the deaths it reviewed. The following tables show the trends over time in the circumstances of death. It should be noted that the Ombudsman’s data shows the information for all notifications received, including deaths that are not investigable, while the data from the CDRC relates only to completed reviews.
Child Death Review Committee up to 30 June 2009 – see Note 1
The figures on the circumstances of death for 2003-04 to 2008-09 relate to cases where the review was finalised by the CDRC during the financial year.
Year |
Accident – |
Accident - Vehicle |
Acquired Illness |
Asphyxiation /Suffocation |
Alleged Homicide (lawful or unlawful) |
Immersion/ Drowning |
SUDI * |
Suicide |
Other |
2003-04 |
1 |
1 |
1 |
1 |
2 |
3 |
1 |
|
|
2004-05 |
|
2 |
1 |
1 |
3 |
1 |
2 |
|
|
2005-06 |
1 |
5 |
|
|
2 |
3 |
13 |
|
|
2006-07 |
1 |
2 |
2 |
|
|
|
4 |
1 |
|
2007-08 |
2 |
1 |
|
|
1 |
1 |
2 |
3 |
4 |
2008-09 |
|
|
|
|
|
1 |
6 |
1 |
|
- * Sudden, unexpected death of an infant – includes Sudden Infant Death Syndrome
Ombudsman from 30 June 2009 – see Note 2
The figures on the circumstances of death from 2009-10 relate to all notifications received by the Ombudsman during the year including cases that are not investigable and are not known to DCPFS. These figures are much larger than previous years as the CDRC only reported on the circumstances of death for the cases that were reviewable and that were finalised during the financial year.
Year |
Accident Other Than Motor Vehicle |
Motor Vehicle Accident |
Illness or Medical Condition |
Asphyxiation /Suffocation |
Alleged Homicide |
Drowning |
SUDI * |
Suicide |
Other |
2009-10 |
4 |
17 |
7 |
|
5 |
5 |
25 |
9 |
4 |
2010-11 |
9 |
22 |
17 |
|
2 |
8 |
34 |
11 |
15 |
2011-12 |
2 |
17 |
11 |
|
4 |
4 |
31 |
11 |
3 |
2012-13 |
8 |
15 |
15 |
|
3 |
12 |
32 |
18 |
3 |
2013-14 |
4 |
15 |
9 |
|
1 |
3 |
26 |
10 |
2 |
2014-15 |
4 |
20 |
14 |
|
|
3 |
28 |
13 |
2 |
* Sudden, unexpected death of an infant – includes Sudden Infant Death Syndrome
Note 1: The source of the CDRC’s data is the CDRC’s Annual Reports for the relevant year. For 2007-08, only partial data is included in the Annual Report. The remainder of the data for 2007-08 and all data for 2008-09 has been obtained from the CDRC’s records transferred to the Ombudsman. Types of circumstances are as used in the CDRC’s Annual Reports.
Note 2: The data for the Ombudsman is based on the notifications received by the Ombudsman during the year. The types of circumstances are as used in the Ombudsman’s Annual Reports. Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available on the circumstances in which the child died.
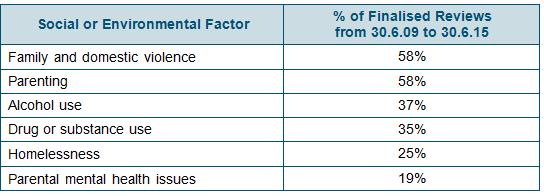
Social and environmental factors associated with investigable deaths
A number of social and environmental factors affecting the child or their family may impact on the wellbeing of the child, such as:
- Family and domestic violence;
- Drug or substance use;
- Alcohol use;
- Parenting;
- Homelessness; and
- Parental mental health issues.
Reviews of investigable deaths often highlight the impact of these factors on the circumstances leading up to the child's death and, where this occurs, these factors are recorded to enable an analysis of patterns and trends to assist in considering ways to prevent or reduce future deaths.
| It is important to note that the existence of these factors is associative. They do not necessarily mean that the removal of this factor would have prevented the death of a child or that the existence of the factor necessarily represents a failure by DCPFS or another public authority. |
One of the features of the investigable deaths reviewed is the co-existence of a number of these social and environmental factors. The following observations can be made:
- Where family and domestic violence was present:
- Parenting was a co-existing factor in nearly three quarters of the cases;
- Drug or substance use was a co-existing factor in over half of the cases;
- Alcohol use was a co-existing factor in over half of the cases;
- Homelessness was a co-existing factor in over a third of the cases; and
- Parental mental health issues were a co-existing factor in almost a quarter of the cases.
- Where alcohol use was present:
- Parenting was a co-existing factor in over three quarters of the cases;
- Family and domestic violence was a co-existing factor in over three quarters of the cases;
- Drug or substance use was a co-existing factor in over half of the cases; and
- Homelessness was a co-existing factor in over a third of the cases.
Reasons for contact with DCPFS
In 2014-15, the majority of children who were known to DCPFS were known because of contact relating to concerns for a child’s wellbeing or for family and domestic violence. Other reasons included financial problems, parental support, access, fostering or adoption enquiries and homelessness.
Patterns and trends of children in particular age groups
In examining the child death notifications by their age groups the Office is able to identify patterns that appear to be linked to childhood developmental phases and associated care needs. This age-related focus has enabled the Office to identify particular characteristics and circumstances of death that have a high incidence in each age group and refine the reviews to examine areas where improvements to public administration may prevent or reduce these child deaths. The following section identifies four groupings of children: under one year (infants); children aged 1 to 5; children aged 6 to 12; and children aged 13 to 17, and demonstrates the learning and outcomes from this age-related focus.
Deaths of infants
Of the 537 child death notifications received by the Ombudsman from 30 June 2009 to 30 June 2015, there were 192 (36%) related to deaths of infants. The characteristics of infants who died are shown in the following chart.
Characteristics of Infants (Children under One Year) |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
Further analysis of the data shows that, for these infant deaths, there was an
over-representation compared to the child population for:
- Males – 74% of investigable infant deaths and 59% of non-investigable infant deaths were male compared to 51% in the child population;
- Aboriginal children – 65% of investigable deaths and 33% of non-investigable deaths were Aboriginal children compared to 6% in the child population; and
- Children living in regional or remote locations – 53% of investigable infant deaths and 43% of non-investigable deaths of infants, living in Western Australia, were children living in regional or remote locations compared to 27% in the child population.
An examination of the patterns and trends of the circumstances of infant deaths showed that of the 192 infant deaths, 175 (91%) were categorised as sudden, unexpected deaths of an infant and the majority of these (115) appear to have occurred while the infant had been placed for sleep. There were a small number of other deaths as shown in the following charts.
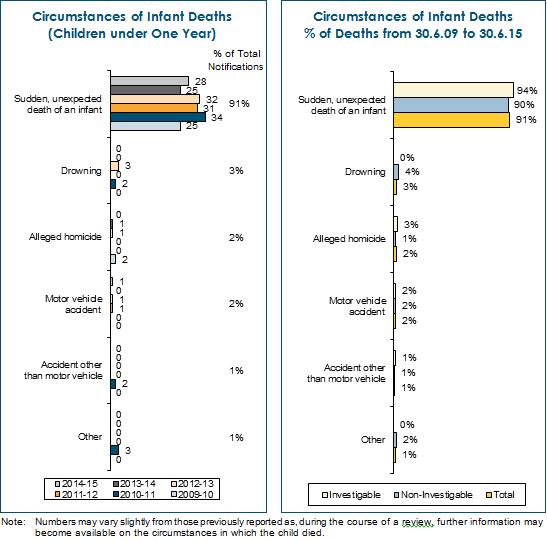
Sixty six deaths of infants were determined to be investigable deaths.
Deaths of children aged 1 to 5 years
Of the 537 child death notifications received by the Ombudsman from 30 June 2009 to 30 June 2015, there were 110 (20%) related to children aged from 1 to 5 years.
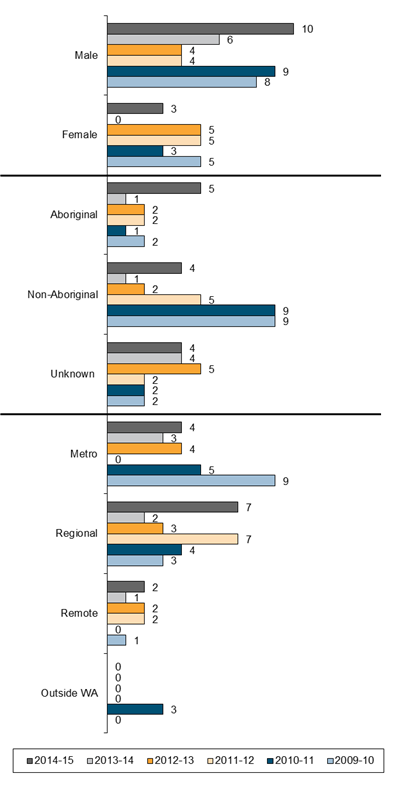
The characteristics of children aged 1 to 5 are shown in the following chart.
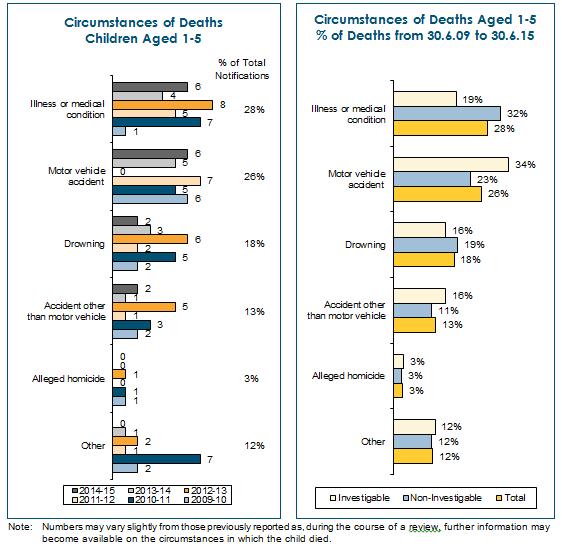
Characteristics of Children Aged 1-5 |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
Further analysis of the data shows that, for these deaths, there was an over-representation compared to the child population for:
- Males – 63% of investigable deaths and 55% of non-investigable deaths of children aged 1 to 5 were male compared to 51% in the child population;
- Aboriginal children – 52% of investigable deaths and 12% of non-investigable deaths of children aged 1 to 5 were Aboriginal children compared to 6% in the child population; and
- Children living in regional or remote locations – 47% of investigable deaths and 41% of non-investigable deaths of children aged 1 to 5, living in Western Australia, were children living in regional or remote locations compared to 27% in the child population.
As shown in the following chart, illness or medical condition is the most common circumstance of death for this age group (28%), followed by motor vehicle accidents (26%) and drowning (18%).
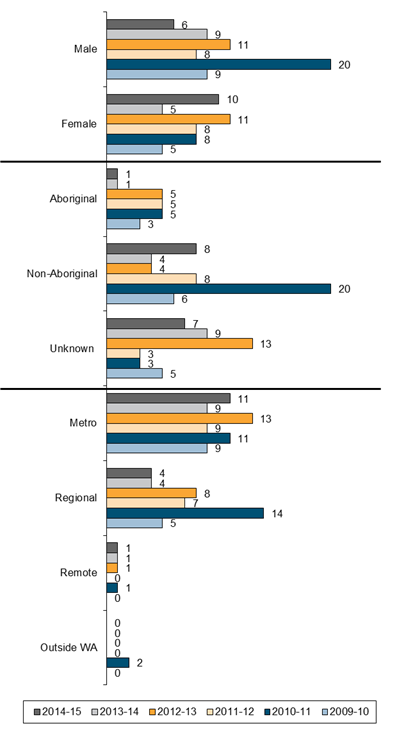
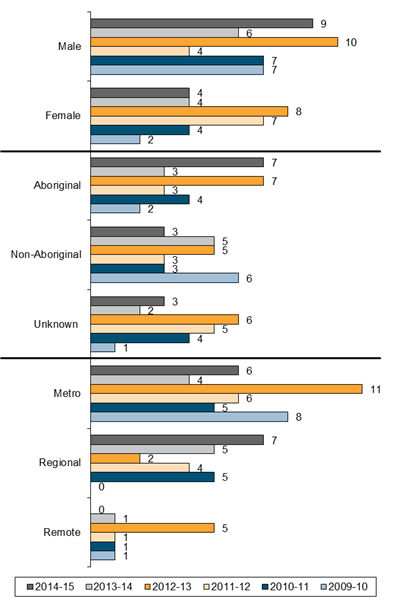
Deaths of children aged 6 to 12 years
Of the 537 child death notifications received by the Ombudsman from 30 June 2009 to 30 June 2015, there were 62 (12%) related to children aged from 6 to 12 years.
The characteristics of children aged 6 to 12 are shown in the following chart.
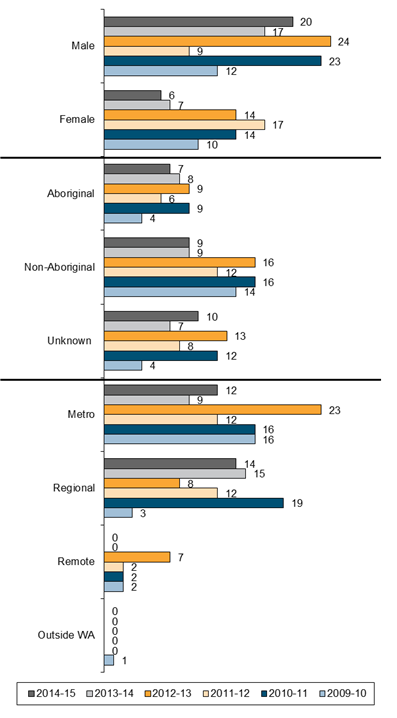
Characteristics of Children Aged 6-12 |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
Further analysis of the data shows that, for these deaths, there was an over-representation compared to the child population for:
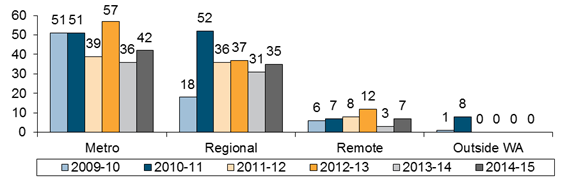
- Males – 57% of investigable deaths and 72% of non-investigable deaths of children aged 6 to 12 were male compared to 51% in the child population;
- Aboriginal children – 48% of investigable deaths and 14% of non-investigable deaths of children aged 6 to 12 were Aboriginal children compared to 6% in the child population; and
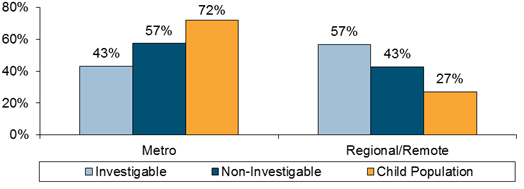
- Children living in regional or remote locations – 70% of investigable deaths and 50% of non-investigable deaths of children aged 6 to 12, living in Western Australia, were children living in regional or remote locations compared to 27% in the child population.
As shown in the following chart, motor vehicle accidents are the most common circumstance of death for this age group (40%), followed by illness or medical condition (28%) and drowning (11%).
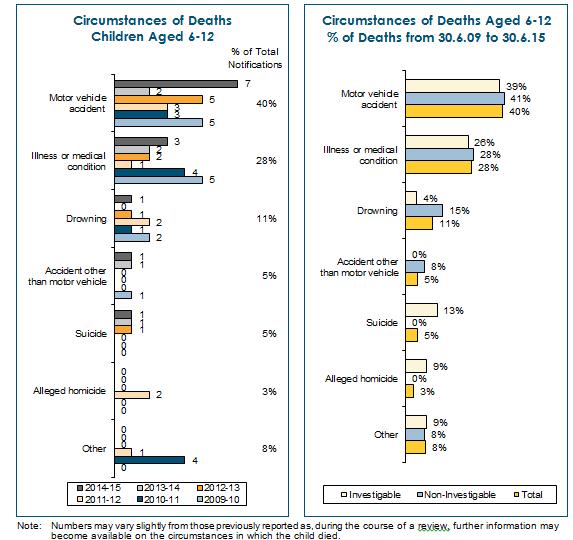
Twenty three deaths of children aged 6 to 12 years were determined to be investigable deaths.
Deaths of children aged 13 – 17 years
Of the 537 child death notifications received by the Ombudsman from 30 June 2009 to 30 June 2015, there were 173 (32%) related to children aged from 13 to 17 years.
The characteristics of children aged 13 to 17 are shown in the following chart.
Characteristics of Children Aged 13-17 |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
Further analysis of the data shows that, for these deaths, there was an over-representation compared to the child population for:
- Males – 55% of investigable deaths and 64% of non-investigable deaths of children aged 13 to 17 were male compared to 51% in the child population;
- Aboriginal children – 55% of investigable deaths and 16% of non-investigable deaths of children aged 13 to 17 were Aboriginal compared to 6% in the child population; and
- Children living in regional or remote locations – 61% of investigable deaths and 41% of non-investigable deaths of children aged 13 to 17, living in Western Australia, were living in regional or remote locations compared to 27% in the child population.
As shown in the following chart, suicide is the most common circumstance of death for this age group (40%), particularly for investigable deaths, followed by motor vehicle accidents (28%) and illness or medical condition (14%).
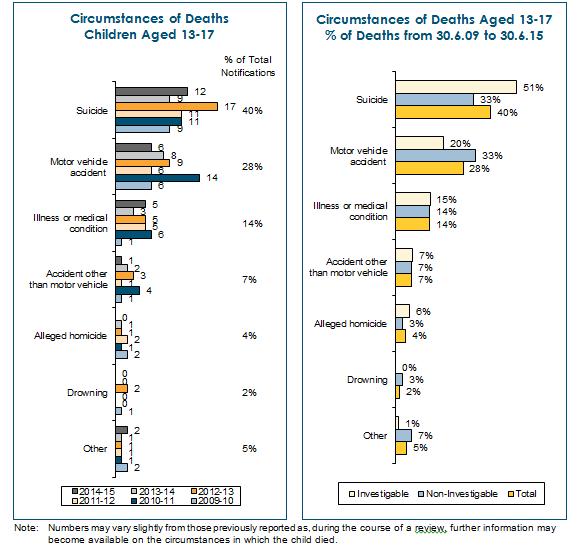
Sixty nine deaths of children aged 13 to 17 years were determined to be investigable deaths.
Suicide by young people
Of the 72 young people who apparently took their own lives from 30 June 2009 to 30 June 2015:
- Three were under 13 years old;
- Four were 13 years old;
- Eight were 14 years old;
- Seventeen were 15 years old;
- Sixteen were 16 years old; and
- Twenty four were 17 years old.
The characteristics of the young people who apparently took their own lives are shown in the following chart.
Characteristics of Young People who Suicide |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
Further analysis of the data shows that, for these deaths, there was an over-representation compared to the child population for:
- Males – 55% of investigable deaths and 65% of non-investigable deaths were male compared to 51% in the child population;
- Aboriginal young people – for the 51 apparent suicides by young people where information on the Aboriginal status of the young person was available, 66% of the investigable deaths and 19% of non-investigable deaths were Aboriginal young people compared to 6% in the child population; and
- Young people living in regional and remote locations – the majority of apparent suicides by young people occurred in the metropolitan area, but 61% of investigable youth suicides and 26% of non-investigable youth suicides were young people who were living in regional or remote locations compared to 27% in the child population.
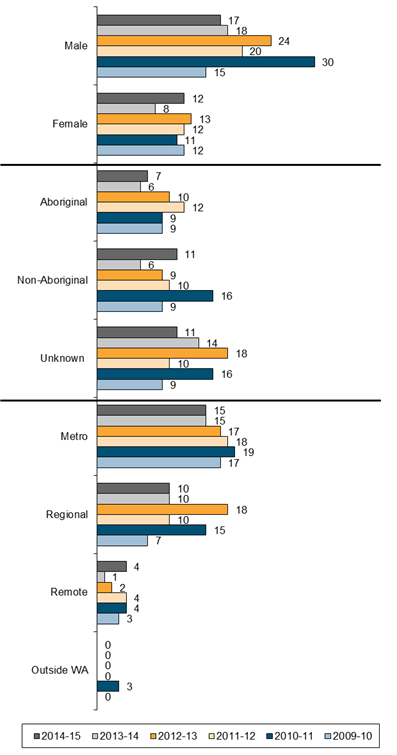
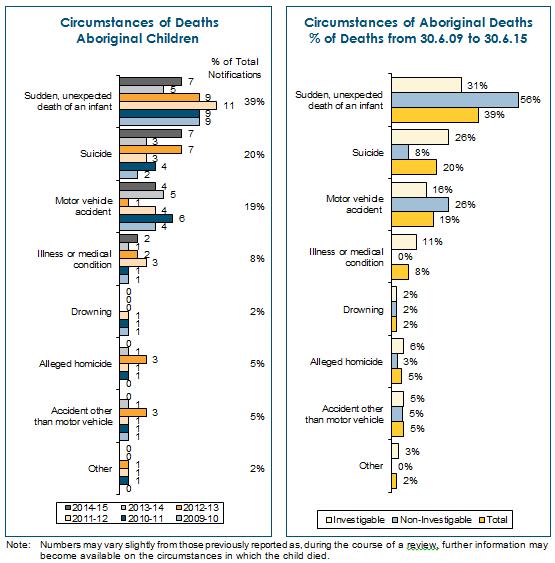
Deaths of Aboriginal children
Of the 346 child death notifications received from 30 June 2009 to 30 June 2015, where the Aboriginal status of the child was known, 129 (37%) of the children were identified as Aboriginal.
For the notifications received, the following chart demonstrates:
- Over the six year period from 30 June 2009 to 30 June 2015, the majority of Aboriginal children who died were male (63%). For 2014-15, 60% of Aboriginal children who died were male;
- Most of the Aboriginal children who died were under the age of one or aged 13-17; and
- The deaths of Aboriginal children living in regional communities far outnumber the deaths of Aboriginal children living in the metropolitan area. Over the six year period, 82% of Aboriginal children who died lived in regional or remote communities.
Characteristics of Aboriginal Children who Died |
|
Note: Numbers may vary slightly from those previously reported as, during the course of a review, further information may become available.
As shown in the following chart, sudden, unexpected deaths of infants (39%), suicide (20%), and motor vehicle accidents (19%) are the largest circumstance of death categories for the 129 Aboriginal child death notifications received in the six years from 30 June 2009 to 30 June 2015.
Improvements to Public Administration to Prevent or Reduce Child Deaths
By undertaking child death reviews the Ombudsman seeks to improve public administration and promote good decision making in those public authorities that provide services to children and families. All improvements are subject to ongoing monitoring and review, to ensure that they are, over time, contributing to the prevention or reduction of child deaths. Information in this section has been set out as follows:
- Issues identified in child death reviews;
- Improvements to public administration to address issues;
- Outcomes of reviews by age cohort;
- Major own motion investigations arising from child death reviews (including future own motion investigations); and
- Other mechanisms to prevent or reduce child deaths.
Issues identified in child death reviews
The following are the types of issues identified when undertaking child death reviews.
It is important to note that:
|
|
Improvements to public administration to address issues
To address the types of issues identified during the Ombudsman’s reviews, the public authorities involved undertook to carry out a range of actions. The following are the types of improvements arising from child death reviews.
|
Outcomes of reviews by age cohort
Information on outcomes of reviews and the administrative improvements achieved as a result of reviews is set out below. The information has been structured under the various age cohorts identified earlier in the patterns and trends section of the report.
Deaths of infants
Sleep-related infant deaths
Through the undertaking of child death reviews, the Office identified a need to undertake an investigation into the number of deaths that had occurred after infants had been placed to sleep, referred to as ‘sleep-related infant deaths’.
The investigation principally involved the Department of Health but also involved the (then) Department for Child Protection and the (then) Department for Communities. The objectives of the investigation were to analyse all sleep-related infant deaths notified to the Office, consider the results of our analysis in conjunction with the relevant research and practice literature, undertake consultation with key stakeholders and, from this analysis, research and consultation, recommend ways the departments could prevent or reduce sleep-related infant deaths.
The investigation found that the Department of Health had undertaken a range of work to contribute to safe sleeping practices in Western Australia, however, there was still important work to be done. This work particularly included establishing a comprehensive statement on safe sleeping that would form the basis for safe sleeping advice to parents, including advice on modifiable risk factors, that is sensitive and appropriate to both Aboriginal and culturally and linguistically diverse communities and is consistently applied state-wide by health care professionals and non-government organisations at the antenatal, hospital-care and post-hospital stages. This statement and concomitant policies and practices should also be adopted, as relevant, by the (then) Department for Child Protection and the (then) Department for Communities.
The investigation also found that a range of risk factors were prominent in sleep-related infant deaths reported to the Office. Most of these risk factors are potentially modifiable and therefore present opportunities for the departments to assist parents, grandparents and carers to modify these risk factors and reduce or prevent sleep-related infant deaths.
The report of the investigation titled Investigation into ways that State Government departments and authorities can prevent or reduce sleep-related infant deaths was tabled in Parliament in November 2012. The report made 23 recommendations about ways to prevent or reduce sleep-related infant deaths, all of which were accepted by the agencies involved.
Each of the recommendations arising from own motion investigations is actively monitored by the Office to ensure its implementation and effectiveness in relation to the observations made in the investigation.
More particularly, significant work was undertaken during the year on a report in relation to the implementation of the Ombudsman’s recommendations arising from the Investigation into ways that State Government departments and authorities can prevent or reduce sleep-related infant deaths.
Deaths of children aged 1 to 5 years
Deaths from drowning
The Royal Life Saving Society – Australia: National Drowning Report 2014 (available at http://www.royallifesaving.com.au/) states (at page 8) that:
Children under five continue to account for a large proportion of drowning deaths in swimming pools, particularly home swimming pools. It is important to ensure that home pools are fenced with a correctly installed compliant pool fence with a self-closing and self-latching gate.
Through the undertaking of child death reviews, including the prevalence of drowning as a circumstance of death for children under one year of age and children between one and five years of age, the Office identified a need to commence, in 2014-15, a major own motion investigation into ways to prevent or reduce child deaths by drowning. The report of this major own motion investigation will be tabled in Parliament in 2016.
Deaths of children aged 6 to 12 years
The Ombudsman’s examination of reviews of deaths of children aged 6 to 12 years has identified the critical nature of certain core health and education needs. Where these children are in the CEO’s care, inter-agency cooperation between DCPFS, the Department of Health and the Department of Education in care planning is necessary to ensure the child’s health and education needs are met.
Care planning for children in the CEO’s care
Through the undertaking of child death reviews, the Office identified a need to undertake an investigation of planning for children in the care of the Chief Executive Officer of the (then) Department for Child Protection – a particularly vulnerable group of children in our community.
This investigation involved the (then) Department for Child Protection, the Department of Health and the Department of Education and considered, among other things, the relevant provisions of the Children and Community Services Act 2004, the internal policies of each of these departments along with the recommendations arising from the Review of the Department for Community Development undertaken by Ms Prudence Ford.
The investigation found that in the five years since the introduction of the Children and Community Services Act 2004, these three agencies had worked cooperatively to operationalise the requirements of the Act. In short, significant and pleasing progress on improved planning for children in care had been achieved, however, there was still work to be done, particularly in relation to the timeliness of preparing care plans and ensuring that care plans fully incorporate health and education needs, other wellbeing issues, the wishes and views of children in care and are regularly reviewed.
The report, titled Planning for children in care: An Ombudsman’s own motion investigation into the administration of the care planning provisions of the Children and Community Services Act 2004, was tabled in Parliament in November 2011.
The report made 23 recommendations that were designed to assist with the work to be done, all of which were agreed by the relevant Departments.
The implementation of the recommendations in the report, and improvement in the ways that public authorities are working to strengthen and enhance care planning for children in the CEO’s care, is actively monitored in individual child death reviews, and through the Ombudsman’s monitoring of the actions taken by public authorities to implement recommendations made by the Ombudsman.
More particularly, significant work was undertaken during the year on a report in relation to the implementation of Ombudsman recommendations arising from the report, Planning for children in care: An Ombudsman’s own motion investigation into the administration of the care planning provisions of the Children and Community Services Act 2004.
Deaths of primary-school aged children from motor vehicle accidents
In 2014-15, the Ombudsman received seven notifications of the deaths of children aged six to 12 years in the circumstances of motor vehicle accidents. In five cases the child who died was a passenger travelling in a car.
The Office of Road Safety’s Fact Sheet Restraints (available at http://www.ors.wa.gov.au/) states at page one:
Drivers and passengers travelling unrestrained in a car are at least 10 times more likely to be killed in a road crash than those wearing a seat belt. Wearing a seat belt may reduce the chance of being killed in a road accident by up to 50%.
In Rural areas 14% of those killed or seriously injured were unrestrained, compared to 5% of those killed or seriously injured in the Metropolitan area.
The Ombudsman’s reviews of these cases identified that of the five children travelling in cars only one notification identified that the child was wearing a seat belt at the time of the accident and four of the five accidents occurred in rural and remote areas.
Deaths of children aged 13 to 17 years
Suicide by young people
Of the child death notifications received by the Office since the commencement of the Office’s child death review responsibility, nearly a third related to children aged 13 to 17 years old. Of these children, suicide was the most common circumstance of death, accounting for nearly 40% of deaths. Furthermore, and of serious concern, Aboriginal children were very significantly over-represented in the number of young people who died by suicide. For these reasons, the Office decided to undertake a major own motion investigation into ways that State Government departments and authorities can prevent or reduce suicide by young people.
The objectives of the investigation were to analyse, in detail, deaths of young people who died by suicide notified to the Office, comprehensively consider the results of this analysis in conjunction with the relevant research and practice literature, undertake consultation with government and non-government stakeholders and, if required, recommend ways that agencies can prevent or reduce suicide by young people.
The Office found that State Government departments and authorities had already undertaken a significant amount of work that aimed to prevent and reduce suicide by young people in Western Australia, however, there was still more work to be done. The Office found that this work included practical opportunities for individual agencies to enhance their provision of services to young people. Critically, as the reasons for suicide by young people are multi-factorial and cross a range of government agencies, the Office also found that this work included the development of a collaborative, inter-agency approach to preventing suicide by young people. In addition to the Office’s findings and recommendations, the comprehensive level of data and analysis contained in the report of the investigation was intended be a valuable new resource for government departments and authorities to inform their planning and work with young people. In particular, the Office’s analysis suggested this planning and work target four groups of young people that the Office identified.
The report, Investigation into ways that State Government departments and authorities can prevent or reduce suicide by young people, was tabled in Parliament in April 2014. The report is available on the Ombudsman’s website.
Arising from the investigation findings, the Ombudsman made 22 recommendations to four government agencies about ways to prevent or reduce suicide by young people, all agreed to by the agencies.
Identification of good practice
Reviews may identify examples of good practice by agencies as shown in the following case study.
Major own motion investigations arising from child death reviews
In addition to taking action on individual child deaths, the Office identifies patterns and trends arising out of child death reviews to inform major own motion investigations that examine the practices of public authorities that provide services to children and their families. During the year, the Ombudsman commenced an own motion investigation into ways that State Government departments and authorities can prevent or reduce child deaths by drowning.
The Office monitors the implementation of recommendations from own motion investigations, including:
- Planning for children in care: An Ombudsman’s own motion investigation into the administration of the care planning provisions of the Children and Community Services Act 2004, which was tabled in Parliament in November 2011;
- Investigation into ways that State Government departments can prevent or reduce sleep-related infants deaths, which was tabled in Parliament in November 2012; and
- Investigation into ways that State Government departments and authorities can prevent or reduce suicide by young people, which was tabled in Parliament in April 2014.
In particular, in 2014-15 the Office undertook significant work on a report on the implementation of recommendations arising from the following two reports:
- Planning for children in care: An Ombudsman’s own motion investigation into the administration of the care planning provisions of the Children and Community Services Act 2004, which was tabled in Parliament in November 2011; and
- Investigation into ways that State Government departments can prevent or reduce sleep-related infants deaths, which was tabled in Parliament in November 2012.
Details of own motion investigations are provided in the Own Motion Investigations and Administrative Improvement section.
Other mechanisms to prevent or reduce child deaths
In addition to reviews of individual child deaths and major own motion investigations, the Office uses a range of other mechanisms to improve public administration with a view to preventing or reducing child deaths. These include:
- Assisting public authorities by providing information about issues that have arisen from child death reviews, and enquiries and complaints received, that may need their immediate attention, including issues relating to the safety of a child’s siblings;
- Through the Ombudsman’s Advisory Panel, and other mechanisms, working with public authorities and communities where children may be at risk to consider child safety issues and potential areas for improvement, and highlight the critical importance of effective liaison and communication between and within public authorities and communities;
- Exchanging information with other accountability and oversight agencies including Ombudsmen in other States to facilitate consistent approaches and shared learning; and
- Undertaking or supporting research that may provide an opportunity to identify good practices that may assist in the prevention or reduction of child deaths.
Stakeholder Liaison
The Department for Child Protection and Family Support
Efficient and effective liaison has been established with DCPFS to support the child death review process and objectives. Regular liaison occurs between the Ombudsman and the Director General of DCPFS, together with regular liaison at senior executive level, to discuss issues raised in child death reviews and how positive change can be achieved. Since the jurisdiction commenced, meetings with DCPFS’s staff have been held in all districts in the metropolitan area, and in regional and remote areas.
The Ombudsman’s Advisory Panel
The Ombudsman’s Advisory Panel (the Panel) is an advisory body established to provide independent advice to the Ombudsman on:
- Issues and trends that fall within the scope of the child death review function;
- Contemporary professional practice relating to the wellbeing of children and their families; and
Issues that impact on the capacity of public sector agencies to ensure the safety and wellbeing of children.
The Panel met four times in 2014-15 and during the year, the following members provided a range of expertise:
- Professor Steve Allsop (Director, National Drug Research Institute of Curtin University);
- Ms Jocelyn Jones (Health Sciences, Curtin University);
- Professor Donna Chung (Head of the Department of Social Work, Curtin University);
- Ms Dorinda Cox (Consultant);
- Ms Angela Hartwig (Women’s Council for Domestic and Family Violence Services WA);
- Ms Victoria Hovane (Consultant); and
- Associate Professor Carolyn Johnson (School of Population Health, University of Western Australia).
Observers from DCPFS, the Department of Health, Department of Aboriginal Affairs, Department of Education, Department of Corrective Services, Department of the Attorney General and Western Australia Police also attended the meetings.
4th Australasian Conference on Child Death Inquiries and Reviews
The Office, together with DCPFS, hosted the 4th Australasian Conference on Child Death Inquiries and Reviews on 6 and 7 November 2014. This year the conference also considered inquiries and reviews of family and domestic violence fatalities.
The conference was officially opened by the Honourable Helen Morton MLC, Minister for Child Protection, and featured opening and closing addresses from the Ombudsman and Emma White, Director General of DCPFS.
This important biennial conference, hosted for the first time in Western Australia, provided a program of national and international leaders in reviews of child deaths, serious injuries to children, and family and domestic violence fatalities.
The conference’s theme, ‘Achieving Outcomes that Make a Difference’, provided delegates with the opportunity to consider a range of topics critical to the success of child death and family and domestic violence fatality reviews. These topics included:
- Challenges and opportunities for enhancing child death review functions;
- Child death review: achieving outcomes that make a difference;
- Leading for learning following a child fatality;
- Creating a culture of learning in safeguarding following a crisis;
- Prevention of youth suicide;
- Child death: the impact of family and domestic violence on Aboriginal women, children and families; and
- Issues and challenges for family and domestic violence fatality review jurisdictions and child protection agencies.
Attendees had the opportunity to participate in discussions about innovations, challenges and future opportunities to strengthen child protection services and child death and family and domestic violence fatality review practices by achieving outcomes that make a difference.
During his opening address, the Ombudsman highlighted the importance of working collaboratively across professional and jurisdictional boundaries to develop expertise in conducting child death reviews and reviews of family and domestic violence fatalities in Australia and New Zealand.
The conference, which received very positive feedback, featured keynote addresses from Professor Donna Chung, Head of the Department of Social Work at Curtin University, and Victoria Hovane, Managing Director of Tjallara Consulting. Former Director General of DCPFS, Terry Murphy, and Jayne Forsdike, from Newcastle Children’s Social Care, also gave presentations to delegates. Copies of all presentation slides are available on the Ombudsman’s website.
Other key stakeholder relationships
There are a number of public authorities and other bodies that interact with, or deliver services to, children and their families. Important stakeholders with which the Office liaises as part of the child death review jurisdiction include:
- The Coroner;
- Public authorities that have involvement with children and their families including:
- Department of Housing;
- Department of Health;
- Department of Education;
- Department of Corrective Services;
- Department of Aboriginal Affairs;
- Western Australia Police; and
- Other accountability and similar agencies including the Commissioner for Children and Young People;
- Non-government organisations; and
- Research institutions including universities.
A Memorandum of Understanding has been established by the Ombudsman with the Commissioner for Children and Young People and a letter of understanding has been established with the Coroner.
Aboriginal and regional communities
Significant work continued throughout the year to build relationships relating to the child death review jurisdiction with Aboriginal and regional communities, for example by communicating with:
- Key public authorities that work in regional areas;
- Non-government organisations that provide key services, such as health services to Aboriginal people; and
- Aboriginal community leaders to increase the awareness of the child death review function and its purpose.
Additional networks and contacts have been established to support effective and efficient child death reviews. This has strengthened the Office’s understanding and knowledge of the issues faced by Aboriginal and regional communities that impact on child and family wellbeing and service delivery in diverse and regional communities.
As part of this work, Office staff liaise with Aboriginal community leaders, Aboriginal Health Services, local governments, regional offices of Western Australia Police, DCPFS and community advocates.
Go to next section of the Annual Report 2014-15 >>
Go to previous section of the Annual Report 2014-15>>
Go back to Annual Reports page >>
Download the Child Death Review section as a PDF
To read a pdf, you will need Adobe Acrobat Reader, which can be downloaded
for free from Adobe at http://www.adobe.com/products/
acrobat/readstep2.html.